



Five evidence-based early known Covid facts - ignored and censored
Highly acclaimed experts presented evidence-based facts on Covid-19 already at the beginning of the crisis in 2020, but were ignored and censored by the authorities

Continued from "Were Covid Measures Based on Science, Part 1"
The official narrative in the Covid crisis tried to persuade the public that various mandates and coercions, limiting people’s individual freedoms, were all based on science. The myth of this has visibly eroded, as it has been revealed how much of the strategies, influencing the lives of millions, was based on fear, pressure from media and political tactics. Reference to science was often enough used as a disguise.
Five evidence-based facts known already in 2020, but ignored by the authorities:
The virus had spread much more widely and was far less dangerous than initially claimed by the authorities.
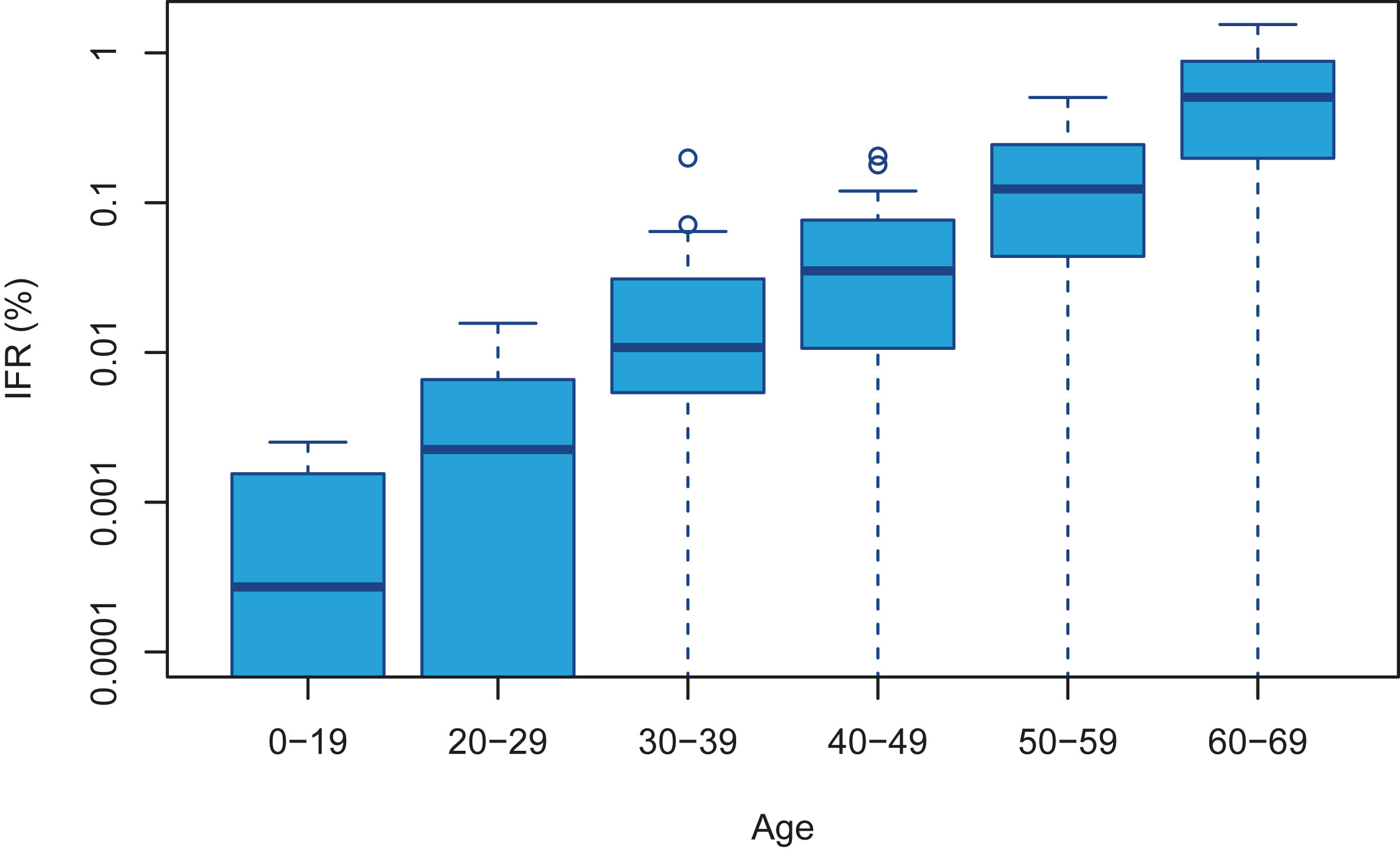
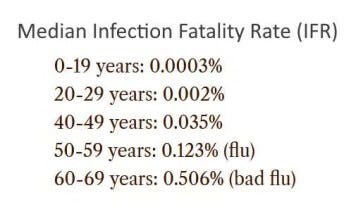
The risk from Covid-19 differed by a factor of 1,000 for different age groups, and the risk was much higher for people with comorbidities (e.g. obesity, diabetes, anxiety disorders, etc.) and nutrition deficiencies.
Those who had recovered from the disease had developed strong natural immunity, but this evidence-based fact was systematically ignored or downplayed by the authorities.
Covid-19 vaccines received marketing authorisation without having been tested in clinical trials for virus transmission or infection.
Covid-19 vaccines have considerable side effects that were already known during the clinical trials of the vaccines.

Already in 2020, there were a number of important and evidence-based facts about both Covid-19 and the response to the Covid crisis that were highlighted by many scientists and doctors. Consideration of these facts would have prevented the introduction of ill-considered and ineffective Covid measures and reduced the resulting harms.
The virus had spread much more widely and was much less dangerous than claimed
The SARS-Cov-2 virus was already much more widespread globally in early 2020 than official sources (including the World Health Organization, or WHO) claimed. Prof. Jayanta Bhattacharya and Eran Bendavid wrote on March 24, 2020, that fears of Covid-19 were based primarily on a miscalculated death toll reported by the WHO, which was vastly exaggerated as it did not take into account the actual rate of infection. This meant, in particular, that the mortality rate among those infected was much lower than initially claimed and the risk posed by Covid-19 to the vast majority of people, particularly those under 70, was many times lower.
A team led by professor John P. Ioannidis of Stanford University scientifically showed in a study published already in May 2020 that the risk of dying from Covid-19 for people under the age of 65, even in pandemic epicentres, was very low, and deaths amongst people under the age of 65 with no comorbidities were remarkably uncommon. They proposed that strategies focusing specifically on protecting high-risk elderly individuals should have been considered in managing the pandemic.
On October 14, 2020, the Bulletin of the World Health Organisation published a study by prof J. P. Ioannidis, according to which the median rate of deaths among people infected with Covid-19 in autumn 2020 was 0.23-0.27%, with a rate of 0.05% among people under 70 years of age, which was tens of times lower than official (including the WHO's) estimates in March and April 2020.
Even though such evidence-based data were known early on, the authorities in many countries and the WHO continued to scare the public about the particular danger of a novel viral disease, and imposed restrictions on millions of healthy people. Among other things, many countries restricted people from exercising, staying outdoors and playing sports, thereby compromising people's overall health and increasing the risk of developing all the diseases (including Covid-19) more severely.
Thousand-fold difference in the risk from Covid-19
Harvard University Professor Martin Kulldorff had already stated in April 2020 that it was clear from the data from Wuhan early on in the crisis that there was a thousand-fold difference in the risk from Covid-19 across different age groups, and that failing to account for this difference was one of the major flaws in the public response to the Covid crisis.

Among people exposed to Covid-19, people in their 70s had roughly twice the mortality of those in their 60s, 10 times the mortality of those in their 50s, 40 times that of those in their 40s, 100 times that of those in their 30s, 300 times that of those in their 20s, and a mortality that was more than 3000 times higher than it was for children. According to Kulldorff, public authorities should have taken this wide variation between age groups into account when designing Covid interventions. Counter measures specifically targeting the elderly, the highest risk group, would have not only protected them but other groups as well. Age-specific measures had to be part of the strategy, otherwise unnecessary mortality, hospital burden and economic losses followed.

Professor Mark Woolhouse of the University of Edinburgh also estimated early on that the elderly were 10,000 times more at risk from Covid-19 than those under 15. But it goes e ven further. It’s not just the elderly, it’s the elderly who are infirm, have comorbidities or are frail. These were the people who were particularly at risk, and the main target group that should have been addressed. In his view, this was also the most important and obvious reason why there were alternatives to social closures and other coercive state measures.
In addition, it was clear from quite early on that it were the people with serious comorbidities that would fall seriously ill. In one of Europe's epicentres of the early outbreak, Italy, a report found as early as in March 20, 2020, that the median age of the 3200 deaths testing positive for Covid-19 was 78.5 years, and more than 95% of them had one or more comorbidities. A large-scale study in the US confirmed that over 95% of hospitalised adults were persons with at least one comorbidity condition and the main risks were obesity, anxiety and fear disorders and diabetes. However, it was also clear, for example, that the proportion of overweight people varied widely between countries, even within the same age groups. For example, obesity already affects 42% of the US population, but in Vietnam the same number is only 2%, in India 4% and <10% in most of the African countries.
The association of nutritional deficiencies with severe morbidity was also known before the Covid crisis. Vitamin D, for example, plays an important role in the immune system. Already in the first half and second half of 2020, studies showed a clear correlation between the low levels of vitamin D and the risk of severe Covid-19 disease. For that reason, many doctors and researchers stressed the need for adequate vitamin D intake in the autumn of 2020, ahead of the second wave, especially for older people at risk.
Although these facts were known early on, authoroties continued to scare the public by claiming, among other things, that the virus did not discriminate between infected people and could be fatal to anyone. Health authorities also failed to advise people to take important steps to support their general health, such as getting enough fresh air and sunshine, eating a healthy diet, controlling blood pressure and diabetes, losing weight, etc. On the contrary, authorities directed people indoors, in many countries penalised them for going outdoors, and just promoted vaccinations instead of various treatments and lifestyles.

Ignoring natural immunity
The importance of natural immunity was systematically downplayed by the health authorities, major vaccine manufacturers and the World Health Organisation (WHO). In some countries (such as the USA), it was not even taken into account in the implementation of Covid measures, while the authorities only reiterated the need to vaccinate as many people as possible.
At the same time, studies carried out before the vaccination campaigns started, i.e. by the end of 2020, clearly showed that recovery from the disease provides strong immunity for at least 8 months and most likely longer. By October 2021, at least 81 studies had already been published confirming immunity to Covid-19 conferred by recovery.

In addition, a number of studies at the beginning of the Covid crisis showed that a significant proportion of the population may have already had immunity to Covid-19, as SARS-Cov-2 was only one of several coronaviruses. Nearly half of the unaffected individuals had the corresponding T-cells, indicating the body's previous exposure to coronaviruses and ability to cope with them.
Many doctors and scientists, including Dr. Robert W. Malone, Dr. Peter McCullough, Dr. Geert Vanden Bossche, Dr Marty Makary, Dr. Pierre Kory, Dr. Tess Lawrie, Dr. Richard Urso, Dr. Paul E. Alexander, Prof Norman Fenton, Prof Martin Neil and others found it puzzling that health officials chose to ignore the scientific fact that infection provided long-lasting and strong protection to millions of people who had recovered from Covid-19. Prof. Jayanta Bhattacharya and Prof. Martin Kulldorff have stressed that while natural infection may not have provided permanent infection-blocking immunity, it offered, in high likelihood, permanent anti-disease immunity against severe disease and death. However, scientists who during the Covid crisis stressed the importance of natural immunity and asked to take into account when divising public policies, were not only ignored but censored and cancelled.

Ignoring natural immunity has had serious consequences, including avoidable vaccine complications and harms, loss of lives, financial and other collateral damage, and loss of credibility of the public health authorities.
Vaccines were not tested for reduction of virus transmission or infection
Covid-19 vaccines, which were introduced at warp speed, were not tested in clinical trials to see if they reduced infection or transmission. Shortly before their vaccine was granted emergency marketing authorisation in the US (on 3 December 2020), this fact was admitted by the CEO of Pfizer, Albert Bourla, and later by a Pfizer official during an official hearing at the European Parliament, although the vaccine manufacturers gave the public an impression that the vaccines protected against infection and transmission.
To the experts who looked closely at the design and results of the Covid-19 vaccine clinical trials, the fact that the vaccines were not tested for reduction of virus transmission or infection was evident already in late 2020. For example, the editor of British Medical Journal (BMJ) Dr. Peter Doshi stated on October 21, 2020, that none of the vaccine clinical trials had been designed to detect the efficacy of these vaccines on reducing any serious outcomes such as hospital admissions, use of intensive care, or deaths. Neither did they examine the efficacy of vaccines for their ability to interrupt transmission of the virus.

Prof. William A. Haseltine drew attention to the serious shortcomings of these clinical trials on 23 September 2020, after Pfizer, Moderna, AstraZeneca and Johnson & Johnson had published their vaccine trial protocols. According to him, the trials seemed to be designed to prove that their vaccines worked, even if the measured effects were minimal, as they mainly investigated only how well could the vaccines prevent mild Covid-19 symptoms. Haseltine pointed out that a closer look at the protocols made it clear that these trials did not provide confidence in vaccine efficacy in protecting against serious illness or in preventing an infection of Covid-19. It also appeared that these trials were intended to pass the lowest possible barrier of success. Haseltine concluded that these vaccines were not the "silver bullet" that would end the Covid crisis.
Yet tens of millions of people around the world were subjected to compulsory vaccination, and many lost their jobs because of non-compliance, severely restricting their individual freedoms and fundamental rights.
Ignoring the side effects of the vaccines
Data on the side effects of the vaccines were already available in documents published by the vaccine manufacturers on their clinical trails in late 2020, although few were able to or considered it important to look at them in depth. This was made considerably more difficult by the fact that vaccine manufacturers refused to publish the raw data needed for an objective assessment. Raw data from clinical trials have still not been fully disclosed.
For example, the Pfizer vaccine trial was designed, conducted, analysed and compiled by Pfizer staff and all the raw data belong to the company. The BMJ editorial board believes that refusing to disclose the original data is morally unacceptable for any clinical trials, but especially those involving major public health interventions. The BMJ has been calling on vaccine manufacturers for years to disclose the original data from clinical trials, since clinical trial data must be available for independent scrutiny.
Nevertheless, experts pointed out many inconsistencies and questionable findings in the Covid-19 vaccine trial reports already in early 2021, such as the facts that:
higher-risk target groups (elderly and immuno-compromised individuals) were clearly under-represented in the trials,
a number of subjects were withdrawn for unknown reasons,
even the officially reported rate of adverse reactions was several times higher than it was, for example, for flu vaccines.

In addition, it has come to light that the vaccine manufacturer Pfizer was aware of several serious side effects amongst the vaccine participants in clinical trials in early 2021, but chose to conceal them, such as the case of 12-year-old Maddie De Garay, who became disabled in the trial and is now partially paralysed, requiring a wheelchair and feeding tube. None of her 35 adverse reactions were mentioned in the New England Journal of Medicine article reporting on the vaccine trial.
Regardless of all that, since the beginning of 2021, mass vaccination campaigns were launched in many countries of the world, which in a short period of time transformed from an attempt of vaccinating the vulnerable target groups (the elderly) into an increasingly massive effort to vaccinate as many people as possible, even up to with children and infants, providing no rational argument or evidence base to do so.
A new expert analysis of the Pfizer and Moderna vaccine trial papers published in 2022 clearly found that participants in these clinical trials were more likely to experience a serious adverse reaction to vaccination than to be hospitalized for Covid-19.
Summary
As shown above, there is ample reason to argue that the evidence base for the decisions made in greatest global health crisis of recent decades was severely deficient. Covid measures were determined not on the basis of evidence nor reasonable assumptions, but rather on the basis of emotional reactions and political tactics, fuelled by fear and media pressure. Societies were under constant pressure from global organisations (WHO, European Commission, etc.), authorities and the mass media - which included the increasingly loud rhetoric of maximizing lockdown, maximizing masking, maximizing vaccination etc.
However, there were also those in power who relied on knowledgeable experts (e.g. in the US, states such as South Dakota, Florida, Texas, etc.), as did some who were in charge of public health institutions (for example in Sweden), succeeding to resist irrational and unscientific pressures while enduring media bashing, vilification and unpopularity. At said places, the decision-makers generally avoided locking down the society and did not impose coercive state measures (compulsory mask mandates, compulsory vaccination, etc.). Thanks to their non-conformist and common sense approach, we now know much about which measures which worked and which didn't, the mistakes every society should avoid in future health crises, and how the slogan of 'follow the science' was often used as propaganda to subjugate societies to the dictates of a line of authority.
We also knew masks were not effective.
Thank you for this excellent summary of the timely, evidence-based information that was ignored. So how did so many people get it so wrong? https://www.hughwillbourn.com/post/23-cock-up-conspiracy-or-murmuration and for a look at the cognitive structure underlying this folly see, "The Bug in our Thinking and the way to fix it" https://www.hughwillbourn.com/book - also on Amazon.